Fertility Success Rates: What They Really Mean
- Feb 25
- 11 min read
Updated: Mar 18

Fertility success rates can quickly become confusing when facing decisions about treatment after 35. For many women with diminished ovarian reserve or unexplained infertility, headline percentages feel hopeful but rarely reflect the reality for your own age and diagnosis. Research shows that most patients significantly overestimate their individual chances compared to what personalized data predict, making accurate information critical. This guide will help you see the real story behind fertility success rates and what matters most when weighing your options.
Table of Contents
Key Takeaways
Point | Details |
Understand Success Rates | Success rates vary widely by clinic and treatment type; always request personalized statistics based on your age and ovarian health. |
Treatment Options Matter | Different fertility treatments have vastly different success rates; know which one aligns best with your specific situation. |
Financial and Emotional Costs | Fertility treatments can be expensive and emotionally taxing; plan your budget and consider your total investment before proceeding. |
Personalized Testing is Key | Comprehensive testing can help identify the best treatment strategy and improve your chances of success per cycle. |
Defining Fertility Success Rates and Misconceptions
Fertility success rates sound straightforward until you actually need to understand them. A clinic reports a 50% success rate, and you naturally wonder: Is that my chance? The answer is far more complicated, and this distinction matters enormously for women over 35 making critical decisions about treatment.
What success rates actually measure varies dramatically between clinics and studies. Most clinics report live birth rates per cycle, but some report pregnancy rates, ongoing pregnancy rates, or cumulative success rates across multiple cycles. The difference is substantial. A pregnancy that ends in miscarriage counts as a success in some statistics but not others.
Population-level statistics mask individual reality. When a fertility clinic publishes a 45% live birth rate, that number represents an average across all patients treated that year. This includes women in their late 20s with excellent egg quality and women in their early 40s with diminished ovarian reserve. Your actual probability depends on your specific circumstances, not the clinic average.
Research shows that most patients significantly overestimate their individual success chances compared to what personalized data predicts. Women often remember the clinic’s headline success rate but ignore how that rate shifts based on age, egg quality, and diagnosis.
Common misconceptions cloud this picture:
Age is not binary. A 36-year-old and a 44-year-old are grouped differently in success rate data, yet clinic statistics often blur these distinctions.
Diminished ovarian reserve changes everything. Success rates for women with normal reserves versus low reserves differ by 30-40 percentage points, yet both groups may receive the same generic statistics.
Multiple cycles compound probability. Success rates per cycle differ dramatically from cumulative success across 3-4 treatment cycles, yet patients often confuse these.
Donor egg success masks your egg quality. If you’re considering your own eggs, a clinic’s overall success rate including donor egg cycles will mislead you.
Your personalized success rate depends on your age, ovarian reserve, diagnosis, and clinic expertise—not the headline statistic you read online.
When evaluating a fertility workup that measures your specific egg quality, you gain the data needed to calculate realistic individual probabilities. This transforms success rates from abstract percentages into personally relevant predictions.
Pro tip: Request your clinic’s success rates specifically for women your age with your diagnosis and ovarian reserve level—this single adjustment often cuts reported success in half, giving you honest expectations rather than inflated hopes.
Types of Fertility Treatments and Calculating Rates
Different fertility treatments produce wildly different success rates, yet most women don’t realize how dramatically treatment choice affects their odds. IVF success rates look nothing like IUI success rates, which look nothing like natural conception rates after surgical correction. Understanding what treatment you’re considering is step one to interpreting your realistic chances.
IVF remains the most studied treatment option. In vitro fertilization produces the highest success rates for women over 35, especially those with diminished ovarian reserve. When clinics report success rates, they’re usually talking about IVF. But IVF isn’t one thing—it’s a category with variations that shift outcomes.
Other major treatment options include:
Intrauterine insemination (IUI) places prepared sperm directly in the uterus, best for cervical factors or mild male factor infertility
Surgical correction for blocked tubes or endometriosis improves natural conception odds without technology
Ovarian rejuvenation therapies aim to enhance egg quality in women with diminished reserves
Donor egg cycles bypass your egg quality entirely, producing substantially higher success rates regardless of age
Success rates vary enormously by treatment type and patient factors. IVF success per cycle ranges from 15-50% depending on age and ovarian reserve, while IUI success per cycle typically stays below 20%. This difference matters when evaluating options.
Here’s how different fertility treatments compare on key factors:
Treatment Type | Typical Success Rate per Cycle | Influenced Most By | Typical Patient Profile |
IVF | 15-50% | Age, ovarian reserve, egg quality | Women over 35, diminished reserve |
IUI | Under 20% | Age, tubal patency, sperm quality | Mild male factor, cervical issues |
Surgical Correction | Varies; improves natural rates | Underlying anatomical problem | Tubal/endometriosis cases |
Donor Egg | Over 50% | Donor egg quality, uterine health | Advanced age or low ovarian reserve |
Ovarian Rejuvenation | Experimental; variable | Ovarian reserve, underlying health | Low reserve, poor responders |
How clinics calculate success rates creates widespread confusion. Three key metrics define IVF success—per cycle, per embryo transfer, and per live birth30424-6/fulltext)—yet reporting standards vary. Some clinics highlight per-transfer rates (higher numbers), while others report per-cycle rates (more conservative). A 45% per-transfer rate becomes 30% when calculated per cycle, yet both numbers are technically correct.
The metric used to calculate success rates can swing your perceived odds by 15-20 percentage points—this is why reporting format matters as much as the actual number.
Cumulative success across multiple cycles provides the most realistic picture for women planning treatment. Your chance of success after three IVF cycles combines those individual probabilities into a more meaningful prediction. Yet many clinics bury cumulative data or don’t calculate it.
Here is a summary of how clinic success rate reporting methods can affect your perception:
Reporting Metric | What It Measures | Typical Reported Rate | Potential Pitfall |
Per Cycle | All started cycles | Lower (e.g., 30%) | Includes all canceled/failed cycles |
Per Embryo Transfer | Only cases with an embryo transferred | Higher (e.g., 45%) | Excludes non-transfer and canceled cycles |
Cumulative (3 Cycles) | Combined rate over three attempts | Highest overall | Not always made clear by clinics |
Age and ovarian reserve create the largest variations within each treatment type. A 36-year-old and a 43-year-old both doing IVF will see dramatically different success rates. This is why generic success rate comparisons fail—you need treatment-specific rates for your exact age and diagnostic category.
Pro tip: Ask your clinic to provide success rates for your specific age group and ovarian reserve level across all three metrics (per cycle, per transfer, and cumulative across three cycles) so you can compare treatments accurately.
Key Factors Influencing Success for Women Over 35
Your age isn’t just a number on success rate charts—it’s the single most powerful predictor of whether fertility treatment will work. Women over 35 face a biological reality that no clinic can ignore, yet understanding exactly why transforms how you evaluate your personal odds.
Age and egg quality are inseparable. Age is the most critical factor determining IVF success, especially for women over 35. This isn’t pessimism; it’s biology. Every month you age, your remaining eggs decline not just in quantity but in quality. Chromosomal abnormalities increase sharply after 35, meaning more embryos fail to develop normally.
Beyond age, several factors shift your individual success rate:
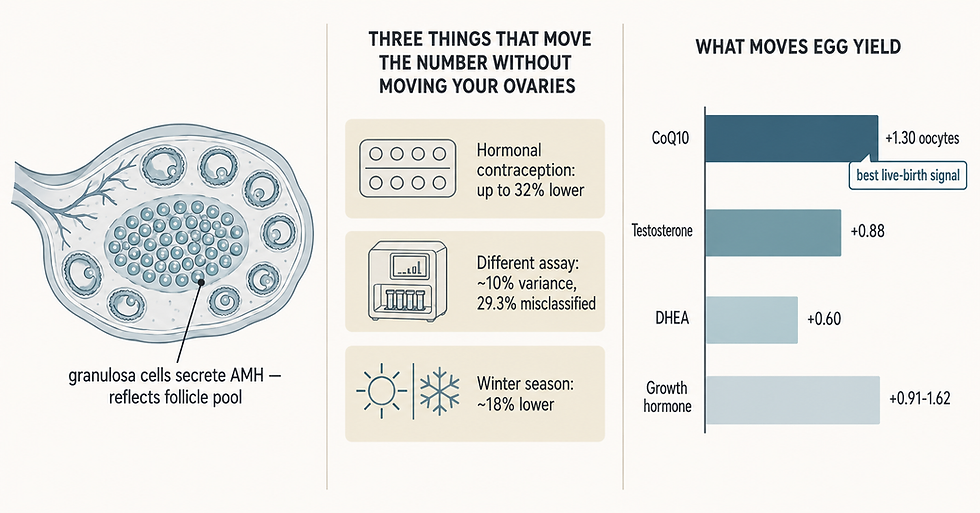
Ovarian reserve markers like AMH and antral follicle count predict how many eggs you’ll retrieve but don’t measure egg quality
Egg quality itself determines embryo development and implantation success, declining faster than most women realize
Uterine receptivity affects implantation odds independent of egg quality
Lifestyle factors including weight, stress, and sleep patterns influence hormone balance and egg quality
Male factor infertility when present reduces success even with your excellent egg quality
Key predictors of IVF success identify egg quality decline and ovarian reserve markers as critical factors for women over 35. Yet clinics rarely distinguish between these two distinct challenges. Low AMH (diminished ovarian reserve) doesn’t automatically mean poor egg quality, but both situations benefit from different treatment strategies.
Age compounds every other factor—a structural uterine problem at 37 differs vastly from the same problem at 44, not because of the uterus but because of the eggs available.
Embryo quality represents the convergence of these factors. Your age determines your egg quality distribution. Your ovarian reserve determines how many eggs you retrieve. Your uterine and immune health determine if embryos implant. Success requires all three working reasonably well.
Diminished ovarian reserve adds complexity for women over 35. If your AMH is low or your antral follicle count is declining, success rates drop further than age alone would predict. Yet ovarian rejuvenation strategies can sometimes improve egg quality and quantity, shifting individual odds when conventional approaches plateau.
Personalized treatment planning matters enormously at this stage of life. Generic protocols designed for average 35-year-olds fail women with specific challenges—whether that’s poor egg quality, structural issues, or immune factors affecting implantation.
Pro tip: Request comprehensive ovarian reserve testing plus embryo quality data from your clinic’s practice to see how women your age with your specific AMH and antral follicle count actually succeed, then compare that to your baseline success expectations.
Understanding Clinic Comparisons and Global Differences
Comparing fertility clinics across countries or even across regions within your country is deceptively difficult. A clinic in Europe reporting 55% success rates looks drastically different from a clinic in North America reporting 42%, yet the difference often reflects reporting standards, not treatment quality. Global disparities in fertility care create apples-to-oranges comparisons that mislead patients making critical decisions.
Reporting standards vary dramatically worldwide. Healthcare policies, demographic factors, and reporting standards affect clinic success rates across regions globally. Some countries mandate transparent reporting to government bodies. Others allow clinics to publish whatever metrics they choose. Some regions exclude failed cycles from their denominator entirely, artificially inflating success rates.
Why clinic comparisons fail in practice:
Patient selection bias varies by region. Clinics accepting only women under 40 report higher rates than clinics serving women with diminished ovarian reserve
Reporting standards differ. One clinic reports live birth per cycle; another reports live birth per transfer, per embryo transferred, or cumulatively
Treatment availability varies. Access to advanced testing, preimplantation genetic testing, and donor eggs shifts success metrics
Healthcare infrastructure affects outcomes. Countries with strong insurance coverage treat different patient populations than out-of-pocket markets
European clinics often report higher success rates than North American clinics for the same patient. This reflects differences in patient acceptance criteria, not necessarily superior medicine. Some European clinics exclude patients over 45 or with AMH below certain thresholds, automatically raising their average success rate.
Patient selection creates the largest difference in reported rates. A clinic serving women with severe male factor infertility reports different success rates than one specializing in donor egg cycles. Neither clinic is better—they’re treating different populations with predictably different outcomes.
Comparing clinics without accounting for patient selection, reporting methods, and treatment scope is like comparing basketball teams by points scored without checking which league they play in.
Global access disparities matter too. Clinics in countries with universal fertility coverage treat patients earlier in their infertility journey, when success rates are higher. Clinics in countries without coverage see patients who’ve already failed multiple cycles elsewhere, naturally producing lower success rates.
When comparing clinics, focus on outcomes for your specific demographic. Request success rates for women your age with your diagnosis, not headline averages. Ask whether they report per-cycle or per-transfer rates. Understand their patient selection criteria. This level of specificity reveals which clinics actually excel for your situation versus which simply report aggressively.
Pro tip: When evaluating clinics globally, request their success rates calculated identically for women your exact age with your specific diagnosis, then ask how their patient population compares to yours—this single adjustment often explains apparent differences more than actual clinical skill.
Costs, Risks, and Maximizing Success Outcomes
Fertility treatment demands both financial and emotional investment, yet most women don’t fully grasp the cost-benefit tradeoff or the actual risks involved. Understanding what you’re paying for and what could go wrong transforms how you evaluate whether treatment makes sense for your situation.
Financial barriers affect treatment access globally. Financial barriers to fertility treatments and strategies to maximize success outcomes require accessible, affordable care and informed decision-making. A single IVF cycle costs $12,000-$20,000 in the United States, while many women need multiple cycles for success. Without insurance coverage, costs compound quickly, forcing difficult decisions about how many attempts are financially feasible.
The financial reality for women over 35:
Single cycle costs don’t reflect total treatment expense; most women need 2-3 cycles to succeed
Testing and monitoring add thousands to the baseline cycle cost
Medication expenses vary based on protocol but typically run $3,000-$6,000 per cycle
Ancillary services like genetic testing, freezing, or storage extend costs significantly
Time off work creates hidden costs many women don’t budget for
Risks associated with fertility treatment require honest discussion. Potential risks include multiple pregnancies and complications specific to IVF, requiring tailored treatment plans and evidence-based decisions. Ovarian hyperstimulation syndrome (OHSS) occurs in 1-2% of cycles but can be serious. Multiple pregnancies carry elevated risks for both mother and babies.
Common treatment risks include:
Ovarian hyperstimulation causing abdominal pain, nausea, and in severe cases, organ complications
Infection or bleeding during egg retrieval, though rare with experienced providers
Multiple pregnancy increasing miscarriage risk and pregnancy complications
Psychological toll from repeated cycles, negative results, and financial stress
The real cost isn’t just dollars—it’s the emotional weight of repeated cycles, the time commitment, and the psychological impact of possible failure.
Maximizing success means strategic planning before treatment begins. Comprehensive testing identifies which treatments actually fit your situation. Some women with unexplained infertility benefit from immune testing or uterine procedures before pursuing IVF. Others need ovarian rejuvenation strategies to improve egg quality rather than standard protocols.
Tailored protocols reduce wasted cycles and costs. A woman with diminished ovarian reserve benefits from different medication doses and timing than a woman with normal reserves. Protocol optimization increases success per cycle, reducing total treatment costs over your fertility journey.
Multiple cycles compound both costs and risks. Success rates improve with each attempt up to about three cycles, then plateau. Understanding your personal threshold—financially and emotionally—matters before starting treatment.
Pro tip: Calculate your total affordable treatment budget, then work backward to determine realistic success odds: ask your clinic your cumulative success rate across three cycles at your specific age and reserve level, then decide if that probability justifies the financial and emotional investment you’re willing to make.
Take Control of Your Fertility Journey with Personalized Care
Understanding fertility success rates can feel overwhelming especially when age, ovarian reserve, and treatment type create so many variables. The truth is your individual chances are unique and require more than generic averages. If you are a woman over 35 or someone facing diminished ovarian reserve, you deserve precise insights and tailored treatment strategies that reflect your specific diagnosis and needs.
At Rejuvenating Fertility Center, we specialize in advanced reproductive medicine designed to maximize your success odds through individualized protocols including IVF with own or donor eggs, ovarian rejuvenation, and comprehensive fertility workups. Do not rely only on broad statistics. Explore how our innovative therapies and expert guidance can empower you to make informed decisions today. Visit our website to learn more and take the first step towards a hopeful future. Your fertility journey deserves care as unique as you are.
Frequently Asked Questions
What do fertility success rates actually measure?
Fertility success rates can differ dramatically between clinics and studies. They may refer to live birth rates, pregnancy rates, ongoing pregnancy rates, or cumulative success rates across multiple cycles. It’s important to understand what metric is being reported for accurate interpretation.
How does age affect fertility success rates?
Age is the most significant predictor of fertility treatment success. As women age, the quality and quantity of their eggs decline, leading to lower success rates. This effect becomes particularly pronounced after age 35.
Why should I ask my clinic for specific success rates?
Requesting success rates specific to your age, diagnosis, and ovarian reserve level gives you a more realistic expectation of treatment outcomes. Generic success rates may not reflect your individual situation, which can significantly differ from the clinic average.
How do different fertility treatments compare in success rates?
Different fertility treatments vary widely in success rates. For example, IVF typically has a higher success rate (15-50%) compared to IUI, which usually remains under 20%. It’s crucial to understand the differences in treatment options to assess your realistic chances of success.
Recommended