
How to Boost AMH Level: What Actually Moves the Number, What Moves Your Odds, and How to Tell the Difference
- 2 hours ago
- 9 min read
Quick answer: Yes — there are real ways to boost your AMH level, and there is good news most articles skip entirely. Before you change anything, check that your number is real. Hormonal birth control can suppress AMH by up to a third, different labs report different values for the identical blood sample, and AMH dips in winter. Once you have a true reading, CoQ10 has the strongest live-birth evidence of any supplement studied, and regenerative options like intraovarian PRP are among the few interventions shown to raise AMH and follicle counts directly. The goal isn't a prettier lab value. It's more eggs — and those are different projects.
What AMH Measures — and Why It Moves
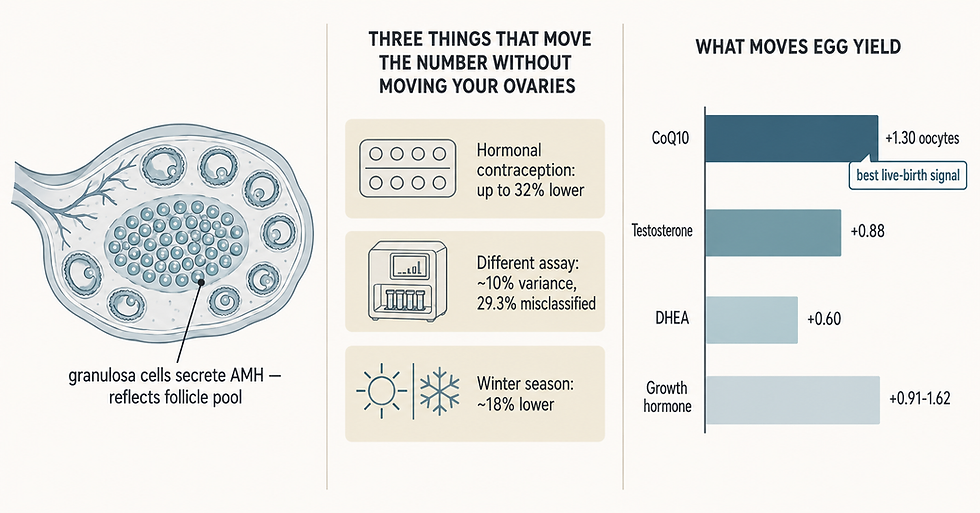
Anti-Müllerian hormone is made by the granulosa cells surrounding your small, early-stage follicles. More follicles in that pool, more AMH in your blood. So AMH is a marker of egg quantity — your remaining reserve.
Search "how to boost AMH level" and you'll get walnuts, DHEA, and a supplement checkout page. Almost none of it starts where it should: with whether the number you're looking at is actually measuring your ovaries.
Because AMH moves for at least three reasons that have nothing to do with your reserve changing. And the women most likely to be affected are, as you'll see, the women most likely to be frightened.
This page is for you if:
You got an AMH result that scared you and want to know what you can actually do
You're planning IVF or egg freezing and want the best possible cycle
You've been told your reserve is low and want options beyond "try donor eggs"
You're comparing supplement claims and want to know which ones have real evidence behind them
Your Low AMH Might Not Be Your Ovaries
This is the part nobody writes, and it's the first thing we check.
Your birth control is suppressing it — possibly a lot
A population study of 42,684 women found hormonal contraception significantly lowers AMH, and the size of the effect depends on the method (Nelson et al., Fertility and Sterility, 2023):
Method | Approximate AMH suppression |
Combined oral contraceptive pill | ~24–32% lower |
Vaginal ring | ~22–65% lower |
Implant | ~23% lower |
Progestin-only pill | ~15% lower |
Hormonal IUD | ~0–7% lower |
Copper IUD | No significant effect |
Now here is the finding that should change how you read your own result. The suppression is strongest at the lowest AMH percentiles. Combined pill use was associated with 32% lower AMH at the 10th percentile — but only 5% lower at the 90th. In plain terms: the women whose numbers look most alarming are precisely the women whose numbers are most distorted.
And it's reversible. Former users show AMH levels similar to women who never used contraception. If you tested on the pill and panicked, you may have panicked at a number that isn't yours.
Your lab's assay changes the answer
AMH values are not interchangeable between labs. The Beckman Coulter assay reads roughly 10% higher than Roche on average — enough that one analysis found 29.3% of women were sorted into the wrong medication dosing category depending on which platform ran the sample (Iliodromiti et al., Human Reproduction, 2017). In the clinically decisive mid-range, agreement between assays drops to only moderate. The Ansh Labs picoAMH assay reads higher than either.
So if your "AMH went up!" or "AMH crashed!" came from two different labs, you may be looking at calibration, not biology. This is exactly why serial values need to come from the same platform — and why a physician who knows which assay produced your number reads it differently than an app does.
Vitamin D and the season
Serum vitamin D correlates positively with AMH, and there's an estimated 18% seasonal decline in AMH over winter that supplementation appears to prevent (Dennis et al., Journal of Clinical Endocrinology and Metabolism, 2012). A February draw and a July draw are not the same test.
None of this means your reserve is fine. It means the first way to "boost" your AMH is to measure it properly — right assay, contraception accounted for, alongside an antral follicle count. That step is free, and it's where we start.
What the Research Shows — What Actually Raises AMH and Egg Yield
Once you have a true number, the question becomes what genuinely helps. Here the evidence is better than the internet's reputation for this topic suggests — but it doesn't reward the things being marketed hardest.
CoQ10 is the standout. A network meta-analysis of adjuvant treatments in poor ovarian response ranked CoQ10 best of all of them for improving live birth rate (OR 2.36, 95% CI 1.07–5.38) (Zhu et al., Reproductive Biology and Endocrinology, 2023). A separate meta-analysis of six randomized trials covering 1,529 women found CoQ10 pretreatment raised clinical pregnancy rates, increased oocytes retrieved by about 1.3, improved embryo quality, and reduced cycle cancellations (Lin et al., Annals of Medicine, 2024). This is a genuine live-birth signal, and it's why CoQ10 is a cornerstone of Rejoova.
Transdermal testosterone was the one intervention associated with improved live birth in a meta-analysis restricted to formally defined diminished ovarian reserve (OR 2.19, 95% CI 1.11–4.32) (Conforti et al., Fertility and Sterility, 2025). DHEA increased oocytes retrieved and embryo implantation rates. Growth hormone raised oocyte yield and clinical pregnancy. Melatonin improved mature oocyte counts and clinical pregnancy.
Intervention | Effect on AMH | Effect on egg yield | Live birth signal |
CoQ10 | Modest increase | +1.30 oocytes (RCTs) | Best of all adjuvants — OR 2.36 |
Transdermal testosterone | Not the endpoint | +0.88 oocytes | OR 2.19 in DOR |
DHEA (75 mg/day) | Modest increase | +0.60 oocytes (RCT) | Not yet demonstrated |
Growth hormone (4–8 IU/day) | Not the endpoint | +0.91–1.62 oocytes | Mixed across analyses |
Melatonin (3 mg/day) | Not well studied | Improved MII oocytes | Not yet demonstrated |
Vitamin D | Corrects seasonal dip | Not well studied | Not yet demonstrated |
Two things jump out. Benefits appear larger after more than two months of use — meaning this is a project you start before a cycle, not the week of. And the supplement with the best evidence is rarely the one being advertised to you.
Boosting the Number vs. Boosting Your Odds
Here's the distinction that will save you time and money.
AMH is a proxy. Nobody's actual goal is a nicer lab value — the goal is more eggs, better embryos, a baby. Those two projects overlap, but they are not the same, and the internet consistently confuses them.
Notice the pattern in the table above. The interventions with the best live-birth evidence — CoQ10, testosterone — are not the ones with the flashiest AMH changes. And a headline like "I doubled my AMH!" tells you very little on its own, because it may be a lab switch, a stopped pill, or summer.
So the useful question isn't "how do I boost my AMH level?" It's "how do I get more usable eggs from the reserve I have?" That's a question about protocol design, adjuvant timing, and whether anything reversible is being missed — which is a physician's job, not a supplement label's.
This is exactly what RFC was built to do. Your antral follicle count, your assay, your contraceptive history, and your response to previous stimulation together tell us far more than a single number ever will. Dr. Merhi's own active research areas are women over 40, low ovarian reserve, and gentle stimulation — and RFC offers three different types of IVF precisely because the right protocol for a low-reserve patient is rarely the maximum dose.
When the Ovary Itself Needs Support
For some women, optimizing a cycle isn't enough — the reserve itself is the obstacle. This is where RFC does work most clinics simply don't offer.
Intraovarian PRP is one of the few interventions shown to move ovarian reserve markers directly. Before-and-after studies report increases in AMH, antral follicle count, and oocytes retrieved (Wang et al., Journal of Clinical Medicine, 2026). Dr. Merhi was the first physician in the United States to develop ovarian PRP protocols for diminished ovarian reserve — this isn't a service RFC added to a menu, it's a protocol he built.
Adipose-PRP ovarian rejuvenation goes further, using adipose-derived stem cells. RFC published world-first research documenting live births in women over 45 using their own eggs following adipose-PRP — work covered by Forbes. RFC also offers Bone Marrow Stem Cell-Enriched PRP, which mobilizes your own bone marrow stem cells to reawaken dormant follicles, and Super Ovarian Rejuvenation.
These are advanced options and they aren't right for everyone — Dr. Merhi assesses candidacy individually. Our guide to ovarian rejuvenation therapies walks through how each one works, and if your cycles have stopped early, our page on premature ovarian failure covers that situation specifically.
What to Expect — Testing, Timeline, and Next Steps

The sequence matters more than the effort. Doing this in the right order saves months.
Establish a true baseline. If you're on hormonal contraception, tell your physician — the number is being read differently. Note which lab and assay ran it. Pair it with an antral follicle count on the same visit.
Correct what's correctable. Vitamin D status is worth checking, particularly in winter.
Start adjuvants early. Benefit appears greater beyond two months of use, so this begins well before a cycle.
Match the protocol to your ovaries. Natural, mini/gentle, or conventional IVF — chosen for your profile, not by default.
Consider regenerative options if indicated. Reviewed individually by Dr. Merhi.
Step | Typical US self-pay range | Timeline |
AMH blood test | $50 – $150 | Any cycle day; results 3–7 days |
Antral follicle count | $150 – $350 | Cycle days 2–5; same-day result |
Vitamin D + full hormone panel | $100 – $300 | Results 3–7 days |
CoQ10 / adjuvant course | Varies | Start 2–3 months before a cycle |
Costs vary by region and coverage; see our pricing page for RFC-specific figures. Diagnostic testing is often covered even when treatment isn't. RFC offers Outside Monitoring, so you can monitor locally wherever you live and still treat with us.
Questions worth asking: Which assay ran my sample, and what is that lab's reference range? Does my antral follicle count agree with my AMH? Is anything reversible suppressing my number? Given my reserve, which of the three IVF types fits me? Am I a candidate for ovarian rejuvenation?
Frequently Asked Questions
How can I boost my AMH level naturally?
Start by confirming the number is accurate — stopping hormonal contraception, using a consistent lab, and correcting a winter vitamin D dip can all change the reading without anything changing in your ovaries. Of the supplements studied, CoQ10 has the strongest evidence, ranking best among adjuvants for live birth. Give it two to three months.
How long does it take to increase AMH levels?
Plan on two to three months. Meta-analyses found effects were more pronounced after more than two months of supplement use, which reflects how long early follicles take to develop. If you stopped the combined pill, values return toward baseline within about two months.
Can birth control cause a falsely low AMH?
Yes — and more than most women realize. Combined oral contraceptives are associated with roughly 24–32% lower AMH, and the vaginal ring can read lower still (Nelson et al., 2023). The effect is largest in women whose AMH is already at the low end, and it reverses after stopping.
Why did my AMH change between two tests?
Often the lab, not you. Assays are not interchangeable — Beckman reads about 10% above Roche, and one analysis found 29.3% of women were classified into a different dosing category depending on the platform. Serial values are only comparable from the same assay.
Does raising AMH mean I'll get pregnant?
Not by itself — AMH is a marker of egg quantity, so what you actually want is more usable eggs. That's why RFC reads your AMH alongside your antral follicle count, your history, and your response to stimulation, and builds the protocol around all of it.
What if my AMH is very low even after a proper workup?
That's the situation RFC specializes in. Options include gentle or natural IVF protocols matched to a smaller reserve, ovarian rejuvenation including PRP and adipose-PRP, bone marrow stem cell-enriched PRP, and our donor egg program, which has a 95% egg thaw survival rate and an 82% clinical pregnancy rate. We have no age cutoff and no weight cutoff.
The Bottom Line
Yes, your AMH can move — but the first and most valuable step in boosting it costs nothing: make sure the number is real before you build a plan around it. Your birth control, your lab's assay, and the season can each shift it more than most supplements will. Once you have a true reading, CoQ10 has the best evidence of anything on the shelf, and there are regenerative options for women whose reserve needs more than a cycle can offer.
If you're holding a low AMH and a lot of conflicting advice, bring it to us. RFC is led by Dr. Zaher Merhi — 110+ peer-reviewed publications, named among the top 2% of scientists worldwide, and the first physician in the US to develop ovarian PRP protocols. Book a consultation and we'll read your number properly, together. You can also explore our egg quality after 40 guide, our fertility supplements guide, or the R&S Longevity Program, where AMH is tracked as one of six measurable clocks.


